Active Learning Conversation around A 17 Year Old Girl with Involuntary Movements And Erratic Speech
This Active Learning Discussion is based on the following original Blog Post by Dr.Preethi :

[7/13, 11:00 AM] PG Post Residency 1: Can any of you solve the questions around this current admitted patient which may become a virtual case for your final exams?
Please check out the generic questions around anatomical location, pathology, etiology and therapeutic options that are standard questions around every patient and let us have your answers here around those
[7/13, 11:01 AM] MBBS UG Student 1: Diagnosis : Acute Rheumatic Fever
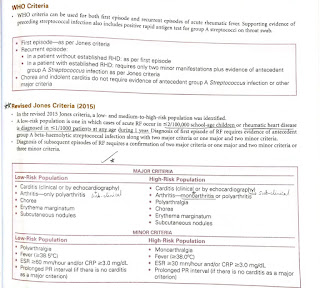
According to the Revised Jones Criteria, our patient satisfies 3 Major criteria (Sydenham's Chorea, Carditis and Subcutaneous Nodules)
Pathogenesis :
-Environmental factors, especially overcrowding leading to repeated group a streptococcal infections in a susceptible host
-Molecular Mimicry
-Streptococcal Superantigens
- Exaggerated T call mediates immune response
Management of Acute Rheumatic Fever : Since it has been more than 6 months since the primary episode of Rheumatic Fever, we need to start the patient on Prophylaxis of initial and recurrent episodes of Rheumatic Fever.
Investigations - WBC Count, ESR, CRP, ECG, Chest x ray, Echo
Treatment -
Primary Prevention -
-Benzathine Penicillin or Oral Penicillin
Secondary Prevention -
-for 5-10 years :
IM inj. Of 1.2 million units of Benzathine penicillin every 3 weeks
Or Oral Penicillin V 500mg twice a day
Or Suphadiazine 1g/day orally as a single dose
Or Erythromycin 250 mg twice a day orally
Or Azithromycin 500mg once a day
Anatomical Localisation :
- Sydenham's Chorea - it is characterised by sudden, aimless, involuntary choreic movements, muscle weakness and emotional instability.
Etiological Localisation :
-Chorea is a delayed manifestation of acute rheumatic fever which is preceded by pharyngeal infection by group A streptococci. Often there is a long latent period of upto 6 months.
Clinical features :
- Jack in the box sign of the tongue
- milking sign /milkmaid's grip
-st. Virus dance
-choriform gait/movements
-pronator sign
-spooning
Management : Complete mental and physical rest, keeping the patient Ina quiet room, padded sideboards for beds to prevent injury, Haloperidol or sodium valproate with diazepam, Rheumatic Fever prophylaxis.
Feature suggestive of Carditis in our patient :
- mild TR
Feature suggestive of Subcutaneous Nodules :
- Small, painless nodules over extensor tendons of hands.
[7/13, 11:13 AM] PG Post Residency 1 : The Echo findings are quite discordant? Can we have moderate to severe PAH with mild TR?
Also what Echo findings in their report is suggestive of rheumatic myocarditis?
Will like to see the video of the findings if available
[7/13, 11:21 AM]MBBS UG Student 1 : Yes sir, the findings seem to be discordant. We cannot have moderate to severe PAH with Mild TR.
[7/13, 11:22 AM] MBBS UG Student 1: The echo video is available on the blog sir
[7/13, 11:24 AM] MBBS UG Student 1: A question - does the patient have to have MR (according to the echo criteria) or is even TR considered?
[7/13, 11:40 AM] PG Post Residency 1: Good question. Please share the Echo criteria of acute rheumatic fever along with the link
[7/13, 11:45 AM]MBBS UG Student 1 : 2012 WHF Echocardiographic criteria for individuals aged ≤20 years
Definite RHD (either A, B, C, or D):
A) Pathological MR and at least two morphological features of RHD of the MV
B) MS mean gradient ≥4 mmHg
C) Pathological AR and at least two morphological features of RHD of the AV
D) Borderline disease of both the AV and MV
Borderline RHD (either A, B, or C):
A) At least two morphological features of RHD of the MV without pathological MR or MS
B) Pathological MR
C)Pathological AR
Normal echocardiographic findings (all of A, B, C, and D):
A) MR that does not meet all four Doppler echocardiographic criteria (physiological MR)
B) AR that does not meet all four Doppler echocardiographic criteria (physiological AR)
C) An isolated morphological feature of RHD of the MV (for example, valvular thickening) without any associated pathological stenosis or regurgitation
D) Morphological feature of RHD of the AV (for example, valvular thickening) without any associated pathological stenosis or regurgitation
[7/13, 11:46 AM] PG Post Residency 1: "MMSE: 19/30 - Moderate MR."
Acute or chronic MR? 🤔
[7/13, 11:47 AM] MBBS UG Student 1: We have to ask the doctor who performed and reported the Echo
[7/13, 11:50 AM] PG Post Residency 1: For which information?
[7/13, 11:51 AM] PG Post Residency 1 : Which Echo criteria for acute rheumatic fever below does this patient satisfy? 🤔
[7/13, 11:52 AM]MBBS UG Student 1: If the MR met all the Echocardiographic criteria for Rheumatic Heart Disease or not.
[7/13, 11:52 AM] PG Post Residency 1 : Your question saved the life of the patient and the PG looking after the patient 😅👍
[7/13, 11:53 AM] PG Post Residency 1: 👆this is a different MR. Mental retardation 😅
[7/13, 11:53 AM] PG Post Residency 1 : None actually
[7/13, 11:54 AM] MBBS UG Student 1: Exactly. I got confused. I remember the patient having TR. I wondered if I missed an MR. 😂
[7/13, 11:56 AM] MBBS UG Student 1: And are we certain the patient has mental retardation? According to what criteria? What if it is a manifestation of her Sydenham's Chorea which presents with emotional and mental instability?
[7/13, 11:58 AM] MBBS UG Student 1: 😅 Thanks, but I don't quite understand how I did that..
[7/13, 12:06 PM] PG Post Residency 1 : You put a spanner in his diagnosis and treatment plan around rheumatic fever 😅
[7/13, 12:06 PM] PG Post Residency 1: 👍
[7/13, 12:06 PM] PG Post Residency 1 : Sydenham chorea causing acute MR?
How common is it for anyone to develop acute MR?
[7/13, 12:07 PM] MBBS UG Student 1: Yes, because one of the Major criteria for Rheumatic fever has to be either Carditis or Arthritis?
[7/13, 12:08 PM] PG Post Residency 1: Behavioral changes, muscle weakness and dysphagia occurred in 70%, 64% and 23% of the patients, respectively. The clinical findings and treatments are summarized in Table 1. (17 patients were included in the study)
[7/13, 12:08 PM] PG Post Residency 1: Which one of these was noticed in your patient? 🤔
[7/13, 12:09 PM] PG Post Residency 1: No it can even be just chorea. Review the current criteria and share what you learn 👍
[7/13, 12:10 PM] PG Post Residency 1: But yes you did some serious damage to the illusion of diagnostic certainty that had been created around this patient 👍😅
[7/13, 12:11 PM]MBBS UG Student 1 : So it can be a combination of ANY of the major criteria? Carditis, Arthritis, Polyarthralgia, Chorea, Erythema Marginatum or Subcutaneous Nodules?
[7/13, 12:17 PM] PG Post Residency 1: Share the link to the current interpretation of Jones criteria
[7/13, 12:18 PM] PG Post Residency 1: The skin lesions also don't look like anywhere near subcutaneous nodules?


[7/13, 12:27 PM] MBBS UG Student 1: The diagnosis of ARF is made on the basis of 2 Major or 1 major and 2 minor or 3 minor criteria ONLY in the presence of evidence of Group A steptococcal infection (Essential Criteria) with the Exception of Sydenham's Chorea
[7/13, 12:28 PM] MBBS UG Student 1: This is because in Sydenham's Chorea, since it occurs almost 6 months after the initial episode of RF, it would not be possible to get raised ASO titres.
[7/13, 12:29 PM] PG Post Residency 1 : 👍
[7/13, 12:30 PM] PG Post Residency 1 : I meant what is the rationale of selecting one major and two minor or two major etc and source
[7/13, 12:32 PM] MBBS UG Student 1: I don't know about this.
[7/13, 12:56 PM]MBBS UG Student 1: But what is the rationale behind any criteria? Why are there criteria anyway? What is the purpose of constructing criteria for various diseases? Who constructs them and on what basis?
[7/13, 1:04 PM] PG Post Residency 1: Yes now you asking the right questions 😅👍
[7/14, 4:48 PM] PG Post Residency 1: Criterias are a net to trap and catch diagnosis.
They are threaded together by data that essentially rests on the principle of incidence of certain events that may correlate with a diagnostic pattern. For example the incidence of having an abnormal choreiform movement in a person with someone exposed to a particular bacteria may correlate with the same person also having a pathology in the joint as well as heart as well as skin that is almost pathognomonic such as aschoffs nodule.
Once a researcher is satisfied that these different events are recurring frequently in the same pattern it sets the ground to define a new diagnosis to the world.
If you keep learning by asking questions one day you too will discover some new patterns that the world doesn't know e
[7/14, 4:49 PM] PG Post Residency 1: yet
[7/14, 4:55 PM] MBBS UG Student 1: Very well explained sir! Thank you 😊
[7/14, 4:56 PM]MBBS UG Student 1 : What about this then?
[7/14, 4:56 PM] PG Post Residency 1: Find out and share what you learn
[7/14, 5:10 PM] MBBS UG Student 1: "Diagnostic criteria are generally broad and must reflect the different features of a disease (heterogeneity), with a view to accurately identify as many people with the condition as possible."
This is all that I could find, sir.
[7/14, 6:44 PM] PG Post Residency 1 : Yes actually it again depends on the same principle of utilizing the correlation of events to snare a diagnostic pattern.
When we use the major and minor combinations, further the major stand for those events that have demonstrated stronger correlation with the diagnostic pattern in the past
Comments
Post a Comment